

Children with hematologic malignancies receiving vincristine chemotherapy are at high risk for developing neuromuscular and musculoskeletal complications [Gohar et al., 2010]. Clinical findings range from sensory disturbances to autonomic dysfunction. Impairments include distal sensory loss in the lower limbs that progress proximally, loss of Achilles tendon reflexes, paresthesias, and loss of proprioception [Vainionpää et al., 1995]. Physical therapy (PT) has been shown to be a helpful intervention in the treatment of chemotherapy-induced peripheral neuropathy (CIPN), with improvement in ankle range of motion and knee extension strength, as well as increases in muscular strength and functional mobility [Gohar et al., 2010; Marchese et al., 2004; San juan et al., 2007]. These studies suggest that physical therapy and exercise rehabilitation can be useful interventions to reduce the adverse side effects associated with CIPN. Early identification and treatment of CIPN may be able to improve the quality of life and functional outcomes in children receiving chemotherapy who are at higher risk of developing decreased strength and impaired mobility. Our aim was to screen for CIPN symptoms in patients with hematologic malignancies receiving vincristine chemotherapy, identify those experiencing significant CIPN, and obtain a baseline assessment on the percentage of patients utilizing PT in the treatment of CIPN.
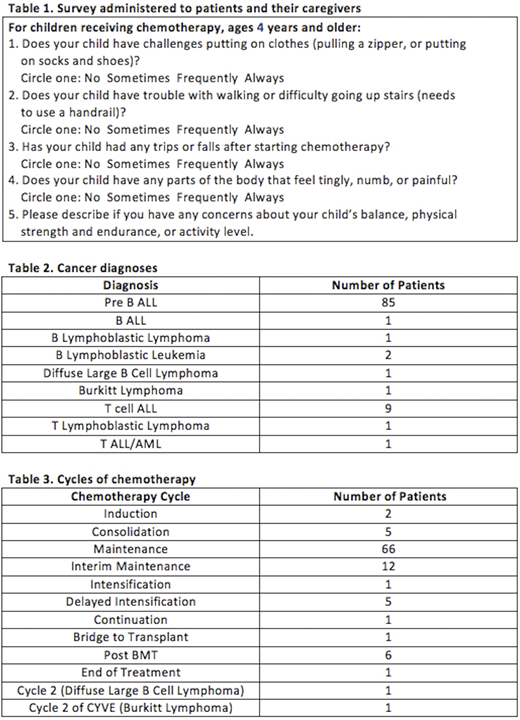
A review of existing medical records of patients who received vincristine at a large regional tertiary care children's hospital was conducted. Surveys (Table 1) assessing CIPN symptoms were administered to patients and their caregivers during clinic appointments during October 2016 through March 2018. Scores from each of the four questions were tallied to obtain a final score indicating severity of patient's symptoms, with a max score of 12. Scores of 1 or greater suggested development of CIPN. Scores between 1 and 3 were considered clinically mild to moderate, and 4 or greater were considered clinically severe.
A total of 116 unique patients participated in the survey, with 102 patients (67 male and 35 female) eligible for analysis. Ages ranged from 4 to 20 years old (4-10 years of age, N = 63; 11-15 years of age, N = 19; 16-20 years of age, N = 20). Cancer diagnoses and cycles of chemotherapy are displayed in Tables 2 and 3. More than half (67.6%, N = 69) of the 102 patients receiving vincristine developed CIPN, of which 16.7% of those 69 patients reported clinically severe symptoms. Common parental concerns noted on the surveys included decreased energy and strength, difficulty walking up and down stairs, limping, increased tripping, and foot drops. However, only 55.1% (38) of the patients who reported CIPN symptoms were referred to outpatient physical therapy; of these patients, 63% (24) set up appointments and utilized the service. A little under half (44.9%, 31) of patients who reported CIPN symptoms on the survey were not referred to outpatient physical therapy. Of the patients who were not referred, 87% (27) had mild to moderate scores of 1-3 and 13% (4) had clinically severe scores of 4 or greater. Approximately one third of all patients received inpatient physical therapy while they were hospitalized during their chemotherapy treatment course.
In this study, we found that a simple survey consisting of 5 questions that only took several minutes to administer identified CIPN symptoms in 67.6% of patients receiving vincristine chemotherapy, which is comparable to 78% of patients with vincristine related neuropathy in the literature [Lavoie smith et al., 2015]. The survey also identified those with CIPN symptoms who were not referred to PT, for reasons possibly attributed to a lack of recognition of CIPN symptoms warranting intervention by the provider, scheduling delays, a limitation of "clean" physical therapy treatment rooms for immunocompromised patients, healthcare visit fatigue, as well as socioeconomic barriers limiting access of care for the patient. Further investigation into the identification of these barriers is important in ensuring that all children and adolescents with CIPN are able to access and utilize physical therapy. Future directions to explore include routine annual screening for development of CIPN, and a study comparing CIPN survey scores of patients before and after physical therapy.
No relevant conflicts of interest to declare.

